
MONDAY, Jan. 16 (HealthDay News) — Gastric bypass surgery results in faster and longer-lasting weight loss than does gastric banding, according to a new study by Swiss investigators.
A gastric bypass operation called Roux-en-Y involves reducing stomach size with staples and connecting the smaller “pouch” directly to the small intestine. It is irreversible.
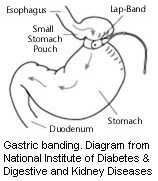
Gastric banding, as its name implies, involves placing a band around part of the stomach to reduce its size. This procedure is reversible, the researchers noted.
“Both gastric banding and gastric bypass are currently performed for morbid obesity,” said lead researcher Dr. Michel Suter, chief surgeon at Chablais Hospital in Aigle.
“Bypass is more effective in terms of directs results such as weight loss, but a bit more dangerous immediately than banding,” he said.
However, banding often leads to long-term complications requiring some sort of major re-operation, Suter said.
“In addition, many bands are not going to stay in place for much more than 10 years; hence, banding is unlikely to be the only weight-loss procedure the patient will be submitted to,” he said. “Patients should make a choice knowing this, and decide whether they accept a slightly higher early risk to improve their results, or if they want the least invasive procedure, but then accept a high risk of further surgery at a later time.”
The report was published in the Jan. 16 online edition of the Archives of Surgery.
For the study, Suter’s team followed for six years 442 patients who had either gastric bypass surgery or banding.
Although there were more early surgical complications among those who had Roux-en-Y surgery, these patients lost more weight faster than those who had gastric banding, the researchers found.
After bypass surgery, about 17 percent of the patients had complications, compared with more than 5 percent of those who underwent banding, the researchers noted.
But at six years there were more problems with gastric banding, including about 48 percent who had weight gain or the procedure reversed, compared with about 12 percent who had bypass surgery, the study found.
Gastric banding was associated with more long-term complications (more than 42 percent versus 19 percent) and more new procedures than bypass surgery (about 27 percent vs. 13 percent).
Cholesterol levels among those who had gastric bypass surgery were consistently lower than among those who had gastric banding, who saw no change over time, the researchers add.
This finding implies that blood sugar levels were also lower among those who underwent gastric bypass surgery, the study authors said.
Suter is concerned that many patients are only offered banding and not told of its drawbacks.
“There is, in the United States, an extensive campaign promoting gastric banding as ‘the solution’ for obesity, which is far from being true,” he said.
It can result in significant weight loss, but it remains a surgical procedure, and is certainly associated with significant risks, both in the short and long term, Suter said.
“Patients must be informed that surgery alone is not sufficient to achieve significant weight loss, and they must be instructed about other things they have to do such as changing their eating and lifestyle habits,” he said.
In addition, Suter said, “Patients calling or referred for gastric banding must be informed about the other available procedures for morbid obesity, and not offered band only, as is the case in several places.”
Depending on the actual operation, either procedure costs between $10,000 and $20,000 plus follow-up costs, and insurance coverage is very inconsistent, according to Dr. Edward Livingston, who serves as the Dr. Lee Hudson-Robert R. Penn Chair in Surgery at the University of Texas Southwestern Medical Center, in Dallas.
Hospital stay for bypass is usually two days, and banding usually one day, but this can vary depending on surgeon, hospital and complications.
Dr. Jacques Himpens, from the European School of Laparoscopic Surgery at Saint Pierre University Hospital in Brussels and author of an accompanying journal editorial, is less concerned with a particular procedure than with the specific surgeon.
“Not all surgeons can do bypasses,” he said. “Maybe they don’t have the skills or the experience, but in any case it’s not the best option because they are not up to it,” he said. “That’s the case for many surgeons.”
In addition, it is not clear what the long-term results of a bypass are, because there is evidence that although a bypass “cures” diabetes, it does come back after time, Himpens said.
“The bypass is a very good procedure, but not everyone can do it and we have to be very careful and watch what the long-term effects of the procedure are,” he said.
Also, while a gastric bypass causes changes in metabolism, banding does not, Himpens said.
“But the good thing is that it is reversible. When you take out the band, no harm has been done and you can still do another procedure if you need to,” he said.
However, among patients who receive bands, only 40 percent retain them after 10 years, either because of complications or the desire to have it removed, Himpens said.
More information
For more on gastric bypass procedures, visit the U.S. National Library of Medicine.